
E-mail senders provided by random name generator at https://www.name-generator.org.uk/quick/.
E-mail senders provided by random name generator at https://www.name-generator.org.uk/quick/.


Click the image to open a larger version in a new window.
You wouldn’t cut the rope of someone rappelling down a mountain, would you? The umbilical cord fulfills a similar lifeline function for a newborn: it delivers oxygenated blood to the baby until Junior’s lungs expand and begin to function. With her usual wisdom, Nature has provided this backup because she knows that newborns do not always breathe immediately. So why the widespread and persistent belief that the cord must be cut, or at least clamped, immediately after birth?The first records of cutting before placental delivery hail from the 17th century. It has been suggested that changes in third stage management accompanied the emergence of male midwives; it became normal practice to deliver women in bed, thereby decreasing the likelihood of spontaneous delivery of the placenta …
In other words, the prone position demanded by new-fangled male birth attendants caused a slower or problematic delivery of the placenta, which then dispensed with the need to wait for the placenta to cut the cord. It makes as much sense as anything else. Providers also believed there to be little benefit in preserving the umbilical cord because the blood flow was so brief:The contribution of the umbilical arteries was considered to be minimal as it was thought that arterial flow stopped within 25–45 s[econds]. However, no explanation for this cessation of flow was provided …2
 One reason that practitioners might have believed blood flow to stop within 45 seconds after birth is that by clamping and cutting the cord immediately after delivery of the newborn, they caused it to stop! Other scientific rationales for early cord cutting included:
One reason that practitioners might have believed blood flow to stop within 45 seconds after birth is that by clamping and cutting the cord immediately after delivery of the newborn, they caused it to stop! Other scientific rationales for early cord cutting included:
 For whatever reason, people seem to fixate on the shoelace. Even Embezzler Home Birth Dad, who surely should know better, feels the need for one. With such depictions so ubiquitous, it’s hardly surprising that parents, first responders, and even medical providers believe that immediate clamping and cutting of the cord is an urgent necessity.
Fortunately, care of the cord following a precipitous birth is remarkably simple: Do nothing.
Want to know more? The 2016 article How to Deliver a Baby (If You Absolutely Have To) provides an excellent set of instructions for supporting a birthing person through a birth in an unplanned location at an unplanned time. We take issue with the headline “You birthed a baby!” since it seems to attribute that accomplishment to the person assisting, rather than to the one who has just produced a new person, but in the face of so much otherwise sound information, we’ll forgive the article’s editors that small oversight.
For whatever reason, people seem to fixate on the shoelace. Even Embezzler Home Birth Dad, who surely should know better, feels the need for one. With such depictions so ubiquitous, it’s hardly surprising that parents, first responders, and even medical providers believe that immediate clamping and cutting of the cord is an urgent necessity.
Fortunately, care of the cord following a precipitous birth is remarkably simple: Do nothing.
Want to know more? The 2016 article How to Deliver a Baby (If You Absolutely Have To) provides an excellent set of instructions for supporting a birthing person through a birth in an unplanned location at an unplanned time. We take issue with the headline “You birthed a baby!” since it seems to attribute that accomplishment to the person assisting, rather than to the one who has just produced a new person, but in the face of so much otherwise sound information, we’ll forgive the article’s editors that small oversight.
 Click the image to open a larger version in a new window.
Click the image to open a larger version in a new window.
As if the U.S. maternity care system didn’t have enough challenges to deal with – a spot of obstetric violence here, a 4-fold racial disparity in maternal mortality there – now there’s that dang Coronavirus! It should come as no surprise that both hospitals and pregnant people might now find themselves with qualms about the practice of giving birth in hospitals.
One potential objection is that healthy people about to give birth might be wary of doing so in a place filled with sick people with a highly contagious disease. The other concern, from the hospital’s point of view, is that facilities and providers might well be strained to the maximum by the exigencies of caring for pandemic patients.
As a result, even parents-to-be who would not have chosen home birth before might find themselves considering it now. It’s not a bad idea! A majority of pregnant people are healthy and are good candidates for home birth. (For comparable safety data on place of birth, see our post here for starters. For more recent data, see the just-released Birth Settings in America report or this summary.) We won’t pretend that hospital-based experts recommend home birth, but others have weighed in on the benefits of separating out healthy mothers and babies from COVID-19 sufferers. None of this is news: in past epidemics, some pregnant hospital patients have switched their planned place of birth.
In order to make out-of-hospital birth possible for many families, however, appropriate providers must  be found to attend those births. The good news is that midwives, particularly Certified Professional Midwives, are currently practicing in almost every state. How those states facilitate access to that care is another matter. CPM practice is legally authorized in 35 states, but each state has different views on CPM scope of practice, Medicaid coverage, and many other issues. In the remaining states, CPM practice exists on a spectrum from unregulated to illegal status.
be found to attend those births. The good news is that midwives, particularly Certified Professional Midwives, are currently practicing in almost every state. How those states facilitate access to that care is another matter. CPM practice is legally authorized in 35 states, but each state has different views on CPM scope of practice, Medicaid coverage, and many other issues. In the remaining states, CPM practice exists on a spectrum from unregulated to illegal status.
If ever there were grounds for support of these maternity care providers who specialize in out-of-hospital care, the COVID-19 pandemic provides it. States must use the emergency police powers available to them to facilitate access to CPMs, and hospital-based medical providers must turn to the important work that only they can do and stop opposing what pregnant people want: the option to give birth in the place of their choosing, attended by a provider of their choice.
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.
Click images to view full-size.



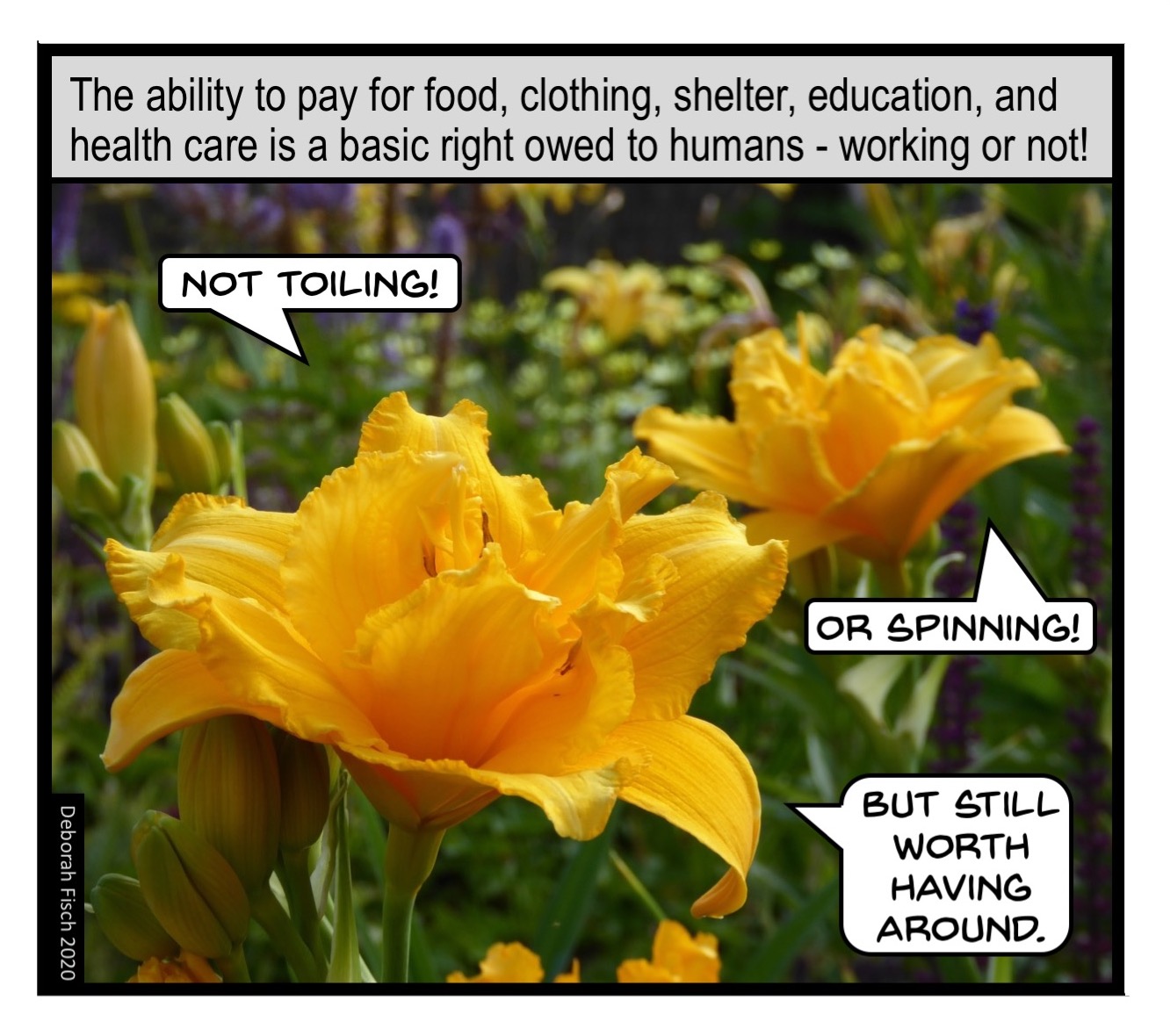
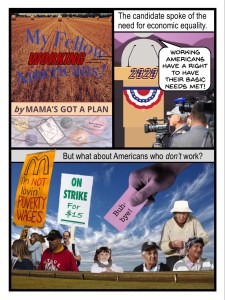
Ah, America the Beautiful. Where good, honest hard work leads – by means of bootstraps – to the bountiful life. That’s a value we can all get behind, yes? Maybe. There are just too many unanswered questions about the nature of work, what constitutes work, and who deserves the rewards of (someone’s) hard work. Give it some thought, and consider whether we don’t all deserve a reasonable measure of security, financial or otherwise, regardless of what occupies our time.
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.
 The two executives celebrating their good fortune are from a photo from pxfuel. They have been placed in a boardroom photographed by Phil Manker. The television image in that photo was added, built on a public domain image by Shealah Craighead.
The two executives celebrating their good fortune are from a photo from pxfuel. They have been placed in a boardroom photographed by Phil Manker. The television image in that photo was added, built on a public domain image by Shealah Craighead.This gallery contains 4 photos
 Click the image to open a larger version in a new window.
Click the image to open a larger version in a new window.
The last few years have seen an increase in states working to decriminalize recreational marijuana use by adults. Apparently, the U.S. Surgeon General believes that only illegal status was preventing pregnant people from puffing their nine months away, because this year he issued a strong warning against marijuana use during pregnancy.
This cartoon addresses criminalization of marijuana use rather than a generalized warning, but the fact is that laws that criminalize drug use during pregnancy and issue special penalties for it already exist and women are being charged under them. Furthermore, even in decriminalized states, mothers still face consequences for marijuana by way of the child welfare system; sanctions can include one that many mothers would rate even worse than the loss of their liberty: the loss of their child. These repercussions seem vastly disproportionate to the drug-using behavior, considering the following facts:
Sanctions, whether threatened or real, scare pregnant people away from prenatal care. When so many things in our lives are bad for babies (job loss, environmental pollution, violence against women), this fixation with a substance whose harm hasn’t even been fully established looks like just another way to criminalize pregnancy. In addition, when marijuana use is legal, punishing users might serve as the bridge to criminalizing tobacco and alcohol use. Or consumption of runny cheese! Or hot tub use. … Or living in a neighborhood where the water has been turned off, homes have been foreclosed upon, and the factory next door belches a queasy-making smoke that the municipality assures residents is Perfectly Safe.
If we want pregnancy to result in healthy babies and healthy mothers, perhaps we might concentrate on known dangers and support parents in ways that don’t involve a) a jail cell, or b) the threat of separation on the single most important day in a brand-new person’s life.
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.



Earlier this year, news articles reported on criminal actions against community (out-of-hospital) midwives in Indiana and Nebraska following infant deaths. More recently, the work of one midwife in Minnesota was highlighted; she was not under state investigation, nor were any bad birth outcomes mentioned.
What do these three midwives have in common? They all have formed Private Membership Associations (PMAs), legal instruments that claim to exempt their members from state regulation. Clients of these midwives become members of PMAs, which supposedly allow them to essentially contract out of state governance of their midwives.
However, in reality it doesn’t work that way. States with licensing regimes, like Indiana, allow their state midwifery boards to issue complaints against negligent midwives, whether the midwives have obtained licenses or not. Because the unlicensed practice of a profession is a criminal offense, these complaints are often conveyed to the state attorney general’s office, after which charges may be filed against the midwife. In states that do not offer licensing of community midwives, like Nebraska, the route to criminal charges is much more direct: reports of a bad outcome may land immediately on the county prosecutor’s desk.
The cartoon above is our take on why PMAs are a bad idea, and why midwife licensing is a good idea. Many people these days mistrust government – and who can blame them? But remember: the answer to bad law isn’t no law; the answer to bad law is good law.
When midwives are arrested after a newborn or maternal demise, as in the news articles linked above, some readers find it tempting to channel their lock-em-up-and-throw-away-the-key rage right at them. Allow us to take this opportunity to remark that physicians rarely face arrest when their patients die. Furthermore, this post is in no way a comment about the outcomes in any of the births in the news articles or on the level of skill and training possessed by the midwives who attended those births. Midwives are often blamed for bad birth outcomes no matter what their license status, training, skill, or education. The shamefully high infant and maternal mortality rates associated with conventional hospital-based care, on the other hand, is just starting to be questioned.
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.
Panel 1:
Panel 2:
Panel 3

All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.

Condemnation is a typical response to mothers who ingest opioids while pregnant. But these women are at risk of receiving much more than a scolding: they may lose their state benefits, their children, and their liberty. Mandatory reporting laws in many states turn health care providers into informants who connect the dots between health care, child welfare authorities, and law enforcement. Reporting of drug-using pregnant people is heavily racialized.
These same health care providers and institutions, however, are content to fix up their laboring patients with epidurals that contain opioids. Epidurals certainly make patients quieter, as the provider in Frame 2 suggests; they are also increasingly demanded by patients who are not permitted to move around during labor, whose contractions have been artificially strengthened with Pitocin, or who are experiencing long labors as a result of physiologic responses to the hospital environment.
Emerging evidence suggests that people exposed to opioids in utero are more likely to develop opioid addictions later in life. We hope that this recognition does not trigger greater retaliation against opioid users who face the sanctions shown in Frame 1, but instead explores all the factors that shape a system that leads to opioid use of any kind by any birthing person.
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.
Very.
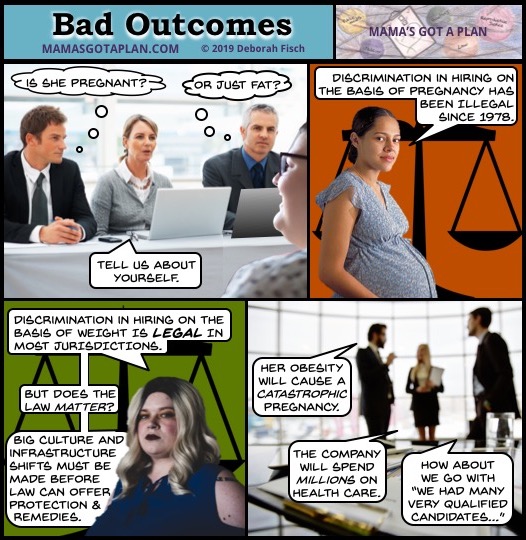
Some women1 are pregnant. Some women are fat.2 Some women are fat and pregnant. Almost all of these women need jobs, the same as anyone else. Employment discrimination in hiring is sadly not unknown to many would-be employees, but the fat-and/or-pregnant job-seeker encounters specific additional challenges.
The Pregnancy Discrimination Act of 1978 forbids employment discrimination on the basis of pregnancy, considering it a form of sex discrimination. The strongest protections apply to the hiring process, but are difficult to access unless an employer documents their decision to discriminate. Employers are not allowed to ask applicants if they have children, plan to have children, or are currently pregnant. Of course, at a certain point a pregnancy becomes visible – unless it is mistaken for fatness.
Discrimination faced by fat people is widespread. Fat people are seen not only as failures at controlling their body size, but also as generally untrustworthy, incompetent, and unhealthy. Most U.S. jurisdictions offer no legal protection against weight-based discrimination in employment or any other context. Even if legal protection were available, remedies might remain elusive should traditional code words for overlooking fat applicants be used: “unprofessional appearance” or “incompatible with company image.” Now for the double whammy …
Yes, Virginia, fat people get pregnant and have babies! It is in these circumstances that employers fall prey to the particularly injurious prejudices about fat people, who are so often characterized as being “one cheeseburger away from a fatal heart attack.” Imagine if a fat person is also pregnant! It’s practically a death sentence! This rate of fatality would be highly inconvenient to employers – not to mention the fat person herself – if it were true.
There are higher risks of some complications of pregnancy associated with higher body weights, but that is true of other (visible) conditions as well: very low body weight, twin or multiple pregnancy, and pregnancy for African-American women, whose maternal mortality is tragically 3-4 times that of white women. The scientific evidence is finally beginning to concede that higher mortality for the African-American population is not the result of race, but of racism. The role of bias and stigma may also be behind the associations of certain types of risk with bad outcomes for fat pregnant women. Regardless of the science, the popular perception is as stated in Frame 4: hiring a pregnant fat woman will bankrupt your business through high health care costs3 when her pregnancy inevitably goes south.
The cultural understanding of women’s participation in the workplace remains far from settled, at least when women take valued positions previously held exclusively by men. Even women who are not pregnant or incapable of becoming pregnant can suffer from employer suspicion that members of the sex that “naturally” acts as family caretakers are likely to be called to do just that, to the detriment of their jobs. Applicants who are pregnant are felt to be freeloading: if other new employees are not permitted to take leave until they have put in the required amount of time, why can babymakers? They should have kept their legs closed!
As for fat pregnant women, well, should they really be permitted to reproduce? Not only will they almost certainly harm their babies and themselves in the process, draining company and public health dollars at an alarming rate, but they might produce more little fat people. A job would just encourage them!
While these last paragraphs are increasingly sardonic in style, they serve to illustrate the result of combining over a century of anti-fat bias, medical eagerness to believe that fat is the cause of all ills, pressure on businesses to reduce health care spending, an economic framework that blames the need of the human race to reproduce on the people doing the reproducing, and a general lack of understanding that we are all in this together. And this moral mess hasn’t even begun to address the additional and intersectional issues encountered by people of color, LGBTQ people, people with disabilities, or immigrants.
You don’t really need us to tell you, do you? Stop discriminating!
Admittedly, it’s not that simple. However, like charity, abuse begins at home – and that’s a good place to stop abusing your fat friends and family members. Even if you’re doing it because you’re “concerned for their health.” Especially then.
Then take up the standard in your workplace. Make sure that both pregnant and fat people are accepted as full members of the workforce. If you are responsible for hiring, then you are especially positioned to make change. Finally, when the common beliefs about fat and/or pregnant people begin to budge, work with policymakers to forbid this kind of discrimination.
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.

At what point do we worry that the sky is falling? At what point is the sky falling? The fear and the actuality can be connected with a line as thin as an EFM trace.
Continuous electronic fetal monitoring (EFM) was introduced to American maternity care in 1970 with the untested promise that it would reduce the incidence of cerebral palsy (CP) by half. CP is a collection of conditions said to be caused by fetal oxygen deprivation during labor and birth. For over 30 years, the scientific community has recognized that EFM has failed to deliver on its promise. Worse than that failure, however, is EFM’s track record of causing an increase in medical interventions, most notably cesarean surgery, which in turn is responsible for increased morbidity and mortality.
Yet EFM is still used in most U.S. births. Furthermore, EFM is so entrenched in hospital practice that true informed consent for its use is rarely given; indeed, patients find themselves almost completely unable to refuse continuous monitoring. How did we get to this place where the standard of care is endangering good care?
| CIRCUMSTANCE | RESULT |
| EFM was put into use six years before the passage of the Medical Device Amendments Act of 1976 that authorized the Food and Drug Administration to begin regulating medical devices. | EFM use was institutionalized with minimal oversight. The lack of regulation allowed EFM manufacturers to grow to an over $2 billion industry. |
| EFM enables nursing staff to track multiple patients from a central bank of monitors, thereby cutting down on staffing that would be required to monitor patients in person. The electronic feed can also be shared with offsite physicians, allowing them to maintain a private practice and carry out other obligations while still caring for their hospital patients. | Staff attention is divided between multiple patients. Patients therefore receive less hands-on attention, allowing abnormalities that may not trigger an abnormal EFM trace to be missed or ignored by providers. Physician interactions with their patients become even more sporadic, sometimes absent until the baby is crowning. |
| Providers view EFM not as an individual procedure with attendant risks and benefits, but as a part of the standard Labor and Delivery package, for which the patient has signed a blanket consent form upon admission. | Patients are not given an opportunity to receive informed consent about EFM use. Since they don’t explicitly consent to EFM, there is no formal opportunity to refuse it. When patients do try to refuse EFM, providers feel tremendous institutional pressure to insist on its use. |
| It was anticipated that EFM would protect practitioners and institutions from medical malpractice liability. The presence of a physical strip (or, nowadays, an electronic file) containing a record of the entire labor, would surely show where physicians acted appropriately. Plaintiff’s attorneys could likewise rely on the strip to show where defendants acted negligently. Unfortunately, the interpretation of EFM signals is notoriously unreliable and variable. | In medmal cases, the EFM strip is now used by both Plaintiff and Defense, with the result that failing to produce a strip in one’s defense is taken as an admission of negligence. Hospital Risk Management departments insist on the use of EFM for potential use in litigation. EFM’s 99% false positive rate remains unacknowledged in courts of law, where dueling experts defend their variable interpretations of the strip. |
| EFM was a new technology that promised to help transcend the barrier of the maternal body, allowing physicians to see more closely what was happening within. | Physicians have come to depend on EFM, not only because of the predictable technological imperative, but also because hand skills, such as abdominal palpation, are no longer taught. |
| The American College of Obstetricians and Gynecologists (ACOG), in its latest practice bulletin on fetal monitoring (#106, 2009), acknowledges all the shortcomings of continuous EFM, including its greater than 99% false positive rate for predicting cerebral palsy and its association with increased instrumental deliveries (forceps and cesarean surgery). Nevertheless, its practice bulletin concludes, “Given that the available data do not show a clear benefit for the use of EFM over intermittent auscultation, either option is acceptable in a patient without complications.” In its latest Committee Opinion (#766, 2019) on “Approaches to Limit Intervention During Labor and Birth” (Committee Opinion #766, 2019), ACOG does not actively recommend replacing EFM, but instead suggests providers consider making arrangements for a hand-held Doppler “for low-risk women who desire such monitoring during labor.” | ACOG’s practice bulletins are subtitled “Clinical Management Guidelines for Obstetrician-Gynecologists.” During litigation, expert witnesses may, depending on specific state law, introduce these guidelines as evidence of standard of care. Because PB 106’s conclusion approves the use of EFM and neglects to note that intermittent auscultation shows a clear benefit over EFM, ACOG’s stance shores up the legal position of EFM use.
The alternate recommendations in CO 766 would be more effective if they were issued in a bulletin that formally replaced PB 106. Since this is not the case, the PB 106 guidelines still stand. |
The factors listed above have contributed to the current EFM impasse: everyone is aware of EFM’s essential defects, but all parties seem united in an emperor-new-clothes fiction that EFM is keeping birthing people and their babies safe. However, as mainstream maternity care begins to focus on reducing non-medically-indicated cesarean surgery in order to rein in the shocking U.S. rate of poor outcomes, most particularly maternal mortality, perhaps EFM will be recognized for its causative role in this situation. We can hope and advocate for appropriate steps that will overcome the barriers to replacing EFM with something more evidence-based, effective, and safe.
This cartoon and post are dedicated to Susan Jenkins, Esq., who created the formulation of risk explained in the final frame, and to Thomas Sartwelle, Esq., who has written extensively on the subject of EFM and was kind enough to share his wisdom at the Birth Rights Bar Association 2019 conference.
“ACOG Committee Opinion No. 766: Approaches to Limit Intervention During Labor and Birth.” Obstetrics & Gynecology 133, no. 2 (February 2019): e164. https://doi.org/10.1097/AOG.0000000000003074.
“ACOG Practice Bulletin No. 106: Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles.” Obstetrics & Gynecology 114, no. 1 (July 2009): 192. https://doi.org/10.1097/AOG.0b013e3181aef106.
Berlatsky, Noah. “The Most Common Childbirth Practice in America Is Unnecessary and Dangerous.” Text. The New Republic, August 13, 2015. http://www.newrepublic.com/article/122532/most-common-childbirth-practice-us-unnecessary-dangerous.
Dekker, Rebecca, and Bertone, Anna. “The Evidence on: Fetal Monitoring.” Evidence Based Birth® (blog), May 21, 2018. https://evidencebasedbirth.com/fetal-monitoring/.
Lent, Margaret. “The Medical and Legal Risks of the Electronic Fetal Monitor.” Stanford Law Review 51 (1999): 33.
Nelson, Karin B., Thomas P. Sartwelle, and Dwight J. Rouse. “Electronic Fetal Monitoring, Cerebral Palsy, and Caesarean Section: Assumptions versus Evidence.” BMJ 355 (December 1, 2016): i6405. https://doi.org/10.1136/bmj.i6405.
Sartwelle, Thomas P., and James C. Johnston. “Cerebral Palsy Litigation: Change Course or Abandon Ship.” Journal of Child Neurology, September 2, 2014. https://doi.org/10.1177/0883073814543306.
———. “Neonatal Encephalopathy 2015: Opportunity Lost and Words Unspoken.” The Journal of Maternal-Fetal & Neonatal Medicine 29, no. 9 (May 2, 2016): 1372–75. https://doi.org/10.3109/14767058.2015.1051526.
Sartwelle, Thomas P. “Defending a Neurologic Birth Injury.” Journal of Legal Medicine 30, no. 2 (June 2, 2009): 181–247. https://doi.org/10.1080/01947640902936522.
———. “Electronic Fetal Monitoring: A Bridge Too Far.” Journal of Legal Medicine 33, no. 3 (July 1, 2012): 313–79. https://doi.org/10.1080/01947648.2012.714321.
———. “Electronic Fetal Monitoring: A Defense Lawyer’s View.” Reviews in Obstetrics and Gynecology 5, no. 3–4 (2012): e121–25.
Sartwelle, Thomas P., James C. Johnston, and Berna Arda. “A Half Century of Electronic Fetal Monitoring and Bioethics: Silence Speaks Louder than Words.” Maternal Health, Neonatology and Perinatology 3, no. 1 (December 2017). https://doi.org/10.1186/s40748-017-0060-2.
———. “The Ethics of Teaching Physicians Electronic Fetal Monitoring: And Now for the Rest of the Story.” The Surgery Journal 03, no. 1 (January 2017): e42–47. https://doi.org/10.1055/s-0037-1599229.
Sartwelle, Thomas P., James C. Johnston, Berna Arda, and Mehila Zebenigus. “Cerebral Palsy, Cesarean Sections, and Electronic Fetal Monitoring: All the Light We Cannot See.” Clinical Ethics, May 24, 2019, 147775091985105. https://doi.org/10.1177/1477750919851055.
Wickham, Sara. “The Case against Electronic Fetal Monitoring | Sarawickham.” Sara Wickham: Midwife, Author, Speaker, Researcher (blog), September 8, 2014. http://www.sarawickham.com/research-updates/the-case-against-electronic-fetal-monitoring/.
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
_(2).jpg){kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}