From the summary page: “This exhibit provides a visual narrative of the emergence and antecedents of reproductive justice. Given that women’s lives have never been reducible to one dimension of their reproductive health, this exhibit traces a longer history of reproductive justice, illustrating many experiences, debates, and policies related to pregnancy, birth, contraception, and raising children. Birthing Reproductive Justice also explores the question of who has produced and controlled knowledge about women’s reproductive health and decisions.
“Installed as a companion to the conference Reproductive Justice: Activists, Advocates, and Academics in Ann Arbor, a Michigan Meeting (May 30-31, 2013), this exhibit showcases materials from the rich and extensive [University of Michigan Libraries collections]. Produced and curated by an inter-campus exhibit team, Birthing Reproductive Justice illustrates the stakes — of physical health, mental health, human dignity, and community empowerment — associated with reproductive justice and suggests that research and advocacy can work together.”
Do public school students have the right to prospectively opt out from encountering a book, specifically one that contains LGBTQ+ materials and themes? Yes, according to SCOTUS, who just decided Mahmoud v. Taylor, in favor of parents who objected to a Maryland school district making books available to teachers and students for classroom use and extracurricular reading. These books were not mandated in classroom curricula. As a result of the decision, parents can demand that their children be pre-emptively opted out from encountering these books. You can read more about the case at Lambda Legal.
We at Mama’s Got a Plan think it’s a grand idea to have books that reflect all students. So here is our review of the seven books in question, complete with spoilers. Wikipedia kindly listed them in grade order … so here we go!
An overwhelmingly happy and rainbow-filled ABC book celebrating many positive values – neighborliness, parades, farmers markets, families, dogs.
This is exactly the sort of book to turn a MAGA brain into whipped cream. So many supportive representations of queerness! We find it pictorially a bit overwhelming, but it is an excellent book to prompt discussion of questions that children may have around LGBTQ identities.
Chloe’s favorite uncle, handsome and endowed with truly beautiful white guy hair (facial and otherwise), announces his engagement to Jamie, to the great delight of the family. Chloe, however, disapproves because marriage would divert Uncle Bobby’s attention away from her. Bobby promises to always love her, and then Bobby and Jamie together charm Chloe with ballet, ice cream sodas, swimming and sailing, and campfires and marshmallows. Chloe yields in the face of their love and attention, allowing Bobby and Jamie to have a picture book (literally!) wedding that everyone enjoys.
This story is not really about gay marriage, but about children dealing with fears of losing the attention of favorite family members who enter new adult relationships. If children cannot stand to see a gay couple in a picture book when the gayness of the couple is not even the theme of the book, they’re going to have a very hard time out in the world once they leave their cloistered community – in which gay couples also exist, if only in the closet.
A thorough explanation of intersectionality and allyship, shown through the eyes of children. Kimberlé Crenshaw, the originator of the intersectionality framework, wrote the foreword. A couple of choice phrases: “We can listen to and support each other in ways that unite us across differences.” “I believe we are strongest when we build communities that are found on the understanding that we have a stake in each other.” Who can argue with that?
A lovely feature of this book is the portrayal of children helping each other, their own families, and one another’s families in situations involving ability status; childcare; gendered clothing and religious garb (hijab); racialized violence (police state); ecology, conservation, and protection of Native Americans; immigrant families, including those fleeing war and violence; language barriers and multilingual families; and citizenship status.
Although listed as a first-grade book, the materials at the end (definitions, notes, and discussion guides) make this an excellent book for children to refer back to as their understanding grows throughout their school years.
Through the lens of Trinity, the main character, who is Black, on the autism spectrum, and a transgender girl, we see examples truly exceptional parenting.
Trinity feels she needs long hair. The problem is that she cannot stand the feeling of her hair growing out. Her family listens carefully but doesn’t know what to do – until cello-playing brother Lucien comes up with the idea of a wig. Her mother takes the idea even further and stays up until the wee hours creating what Trinity needs. The book concludes with a very happy Trinity and the family expressing love. This one made us sniffle. The book shows the reader that when there aren’t simple solutions, with enough love and creativity and dedication people can find the answer.
In addition, this book engages all the senses with its vibrant illustrations and music running behind the words.
The King and Queen feel that Prince – again with the gorgeous hair! – won’t be able to govern alone: the kingdom is simply too big. They travel far and wide to introduce him to various ladies, but “it was soon clear that he was singing a different tune.” When news comes to them that a dragon is threatening the kingdom, Prince races home on his horse. When he is just about to engage the dragon, a knight appears and temporarily blinds the dragon with his shining armor. Prince climbs on top of the beast and subdues it, but in the process is knocked off. Dragons are big, so it’s a long fall, but Knight races on his horse just in time to catch Prince – very romantic! Knight is revealed to be another hot guy with gorgeous hair, and the two men immediately fall in love. Upon returning home, the two lovebirds are accepted and celebrated by the entire community.
This was our least favorite of these books. It is a problematic time to be celebrating monarchy, especially when non-royalty (here, the villagers) are consigned solely to fearing the dragon or cheering Prince and Knight. We don’t really get to know anyone – we don’t even learn Prince’s name! But more importantly, the conflict in this story – Prince’s gayness – is shown as simple and simply solved, which even third-graders will identify as improbable. It’s all very Disney-like, but without challenging any of the foundational beliefs that underlie Disney. The illustrations are Disney-simple too. Perhaps this is a good alternative in a fictional universe filled with Snow Whites and Cinderellas, but we wanted more.
Violet likes her classmate Mira, who shows every sign of liking her back, but Violet is too shy to tell Mira or even accept Mira’s invitations to play together. To explain her feelings, Violet makes Mira a sparkly, glittery Valentine, but cannot bring herself to deliver it. As in a standard rom-com, Violet is clumsy and tongue-tied, earning the mockery of her classmates – who frankly sound like a bunch of hooligans who should be kept in at recess and required to write “I will behave like a mensch” 500 times. Is it Violet’s hint of mannish dressing that sparks their cruelty? This is never addressed. In the end, Violet and Mira exchanges Valentines and become the best of friends.
It’s a sweet story and the illustrations are dynamic. But again, the problem is simple and the solution equally so. Where are the parents? The teachers? The neighbors? Lord of the Flies it isn’t, but the story conveys a sense of isolation and hopelessness in the way the schoolchildren interact. We want a larger conversation about how to bring all the children along, not just a love/like story.
In the middle of a busy family, Penelope knows himself to be a boy. In frustration at not being seen, he misbehaves until his mother discovers his feelings. At first she responds insufficiently, telling him that whatever he feels on the inside is fine. Penelope responds that he doesn’t feel like a boy, he is a boy. To her credit, his mother not only validates him, but makes a plan to tell everyone. Penelope: “For the first time, my insides don’t feel like fire. They feel like warm, golden love.” Again, sniffle! Penelope gets the short haircut he wants, and his mother follows through at his birthday party by explaining his new identity to his grandfather from Ghana. Grandpa responds that in his native language, there are no gendered pronouns – “…gender isn’t such a big deal.” Score! However, the story is not over. Older Brother doesn’t believe Penelope can become a boy just by saying so. Mama wisely explains that not everything has to make sense. “This is about love.”
At school, Penelope wears his boy’s uniform and his status is acknowledged by his friends. In an endearing interchange, the principal asks Penelope if he is a boy, and when he confirms the change, the principal says, “Well, Penelope … today you’re my teacher.” The book concludes with Penelope studying karate and owning his power.
This is more like it! Everyone is involved in Penelope’s decision – his immediate family, his grandfather, his schoolmates, his principal. Just as in My Rainbow, this is a portrait of a loving Black family who knows when to stop and listen, and who understands that a decision about identity is not made in isolation, but in community. We loved this book!
CONCLUSION
These seven books all have something to recommend them, although it should be clear from our reviews where our preferences lie. In addition to depictions of LGBTQ individuals and families, most of the books featured excellent representations of varied abled status, race and ethnicity, and age. Most could use improvement in depictions of different body shapes and sizes.
The parents who brought this lawsuit and the justices who found for the parents are, in our opinion, short-sighted at the very least and bigoted and hateful at the worst. In our own schooldays, did we encounter books that did not reflect our family’s religious, moral, and political views? Yes, pretty much everything in the Western canon! However, the point of education is not that students avoid encountering material they disagree with, but that they experience a broad array of materials while developing critical thinking skills so they can evaluate materials in light of their own and their families’ principles, as well as by diverse standards of quality.
We urge you to sample these books! Visit your local library to request the acquisition of these titles if they are not already in the collection, explore interlibrary loan options, and patronize local independently-owned booksellers.
As the Dobbs regime succeeds Roe, the flames creep closer to everyone.
Click image to open larger version in new window.
The end of an era
With this year’s decision in Dobbs v. Jackson Women’s Health Organization, SCOTUS has ended an era that began with Roe v. Wade in 1973. The action to which the decision has spurred outraged Americans is a silver lining, especially as activist energy extends to other legal regimes deserving of attention. Voting rights? Immigration law? Responses to climate change? One can hope. Without undervaluing the importance of abortion rights, however, we can also admit that Roe, as well as its subsequent line of cases, was not without problems.
Roe‘s problems
The decision’s grounding in the right to privacy, as pulled from the Bill of Rights – or thin air, as per opponents – did not offer the soundest protection. (For other theories of abortion rights, see here. For an examination of privacy and poverty, see this book by the brilliant Khiara Bridges.) Roe also contained language that placed at least some decision-making capacity In the hands of the physician rather than the pregnant person, and used a trimester measurement that reflected only a chronological marker rather than a substantive reason for restricting abortion. It took no notice of the existing uneven access to abortion, similar to access to other health care services. In 1992, Casey v. Planned Parenthood replaced the trimester measurement with “viability,” a moving target due to ever-improving medical developments to treat the neonate. Casey introduced a new legal standard: states were not permitted to restrict abortion for pre-viability pregnancies in ways that presented an “undue burden.” However, subsequent cases failed to rule out most restrictions as undue burdens. Pregnant people apparently suffered no undue burden by being forced to travel long distances with a forced overnight stay so that they might be read a state-mandated script on the alleged risks of abortion and then wait 24 hours to let it sink in before their procedure might begin. In many states, access to abortion under Roe and then Casey was no cakewalk.
Roe‘s OTHER problems
Equally onerous, but much less remarked by the pro-choice movement, was Roe’s misapplication to pregnant people who wanted to continue their pregnancies. How did that work? Roe granted states an increasing “interest in the fetus” over time: states were granted the ability to restrict abortion the farther a pregnancy advanced. Unfortunately, various segments of law enforcement and the judiciary misinterpreted abortion law to mean that states also had an interest – that is, a right to interfere – in pregnancies carried to term. The result has been any number of state interventions, from railroading pregnant people into cesarean surgery, threatening them with child abuse and neglect investigations for failing to fall in line with medical recommendations, all the way to the criminalization of pregnancy, in which Black and Brown people especially are prosecuted if they are found to have used drugs and/or their pregnancies do not result in a perfectly healthy child, even lacking any evidential causal relationship between the two circumstances.
Roe’s demise, far from removing this misapplication, shifts it earlier in the pregnancy. Who can say now when the state’s interest in the prenate begins? When, in fact, does the prenate’s life begin? (That question is examined in this post.) And how early in the life of a person with even the appearance of a future capacity for pregnancy might the state step in? What might the state do now to maintain control over reproduction while continuing to feed the racist prison-industrial complex?
Lace up those boxing gloves!
The moral of this story: Pregnant people possess a common interest, whether they intend to terminate their pregancies or carry them to term. It is in the interest of anyone with a desire to protect reproductive rights, whether that be the right to have children, the right not to have children, and the right to raise children in safety and with dignity, to fight like hell against legal regimes that allow the state to impose restrictions for which pregnant people will bear the consequences.
Image credits
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.
Abortion, and whether it’s good or bad to have one.
Vaccines, and whether it’s good or bad to have one.
People will and do differ on these questions. This cartoon assumes that you want to do the good thing, whatever that is, and that a bad thing is mistreatment or exploitation of people of Color based on racism, whether intentional or not. Are we clear?
<a href="https://mamasgotaplan.com/wp-content/uploads/2021/06/210609-one-moral-concern.jpg" alt="C" width="1018" ><img="" class="wp-image-2081 size-full aligncenter" style="margin-bottom: 0;" title="CLICK TO ENLARGE!" Some people with concerns about the safety or efficacy of vaccines object to the presence of “aborted fetal cells” in vaccines. However easy (and gruesome!) it is to picture a dismembered hand pushing up through a syringe’s liquid, that is not the reality. As the blue-jacketed person in Frame 3 tries to point out, what is in question are cell lines. How are cell lines formed? Scientists use cells taken from an organism, e.g. kidney cells taken from a dead human embryo, and create a replicating cell line. The original kidney cells eventually die off, just as cells in the body do, and are replaced by genetically identical cells created by standard biological cell division. These cells are then combined with viruses and used to create a vaccine. (For fascinating photos of human embryonic stem cells, see here.)
Given this significant distance in both time and nature between embryo and vaccine, what are the moral and practical grounds for boycotting the vaccine because of this association? Those who wish to discourage abortion will not do so by refusing vaccines; the abortions that created the cell lines involved took place decades ago. Should a scientist decide to create a new cell line from embryonic material, current U.S. ethical rules1 forbid the solicitation of pregnant people to terminate pregnancies for the purpose of supplying material for scientific research. People will no doubt continue to terminate pregnancies and the products of conception might subsequently be donated to science, but disrupting that relationship will not prevent abortions.
Do boycotts ever work?
1979 divestment protest, University of Michigan
Boycotts have been effective in other circumstances. Starting in the 1970s, a divestment movement demanded that global institutions isolate South Africa from external trade and investment as a way of pressuring the regime to break down its racial Apartheid system. It worked! South African carried out reforms, a civil war was averted, a Truth and Reconciliation commission took place, and eventually Nelson Mandela became president. By the mid-1990s, Apartheid was no more. In South Africa’s case, the objectionable behavior – the subjugation of a majority of the citizenry – was ongoing. The intense financial pressure applied in the boycott served as an incentive for the government to change its behavior.
Harm that can be redressed – but how?
Other wrongs, however, remain to be righted: consider the case of Henrietta Lacks. The HeLa cell line was developed from cells taken from the cervical tumor that killed Lacks in 1951. The line has been successfully used for far-reaching discoveries in cancer drugs, space research, and immunology, including in the study of COVID-19 in search for a vaccine. The moral issue arises from the fact that while great good came of the establishment of the line, none of that good was directed specifically toward the Lacks family.
The cell line was created from cells taken from Henrietta Lacks, all without the knowledge or permission of the the Lacks family. This practice was and is perfectly legal, as validated by a 1990 California case: the court found that patients do not own any blood or tissue samples taken from their bodies, nor do they possess a right to share in profits from research activities that made use of those samples. However, in HeLa’s case it is difficult for us to ignore the vast gulf between the sums generated by the cell line and the reality of the lives of the Lacks family, who were African-American tobacco farmers in Virginia at a time of blatant racial discrimination. Because such inequalities continue and magnify down through the generations, this injury can be considered an ongoing one.
Should we refuse COVID vaccines because of what was done to the family of Henrietta Lacks? The last panel of the cartoon shows the absurdity of such a proposal: even if it were possible to discard the findings of the space program (!), how would such an action help the Lacks family?
Restorative justice
Let’s try that again.
The concept and practice of Restorative Justice provides a way to compensate victims of injustice, while simultaneously working to prevent future similar injustices. Once used primarily as an alternative within the criminal justice system to address individual instances of property crime, Restorative Justice is now beginning to be deployed more broadly to tackle systemic injustice and inequity.2 The Restorative Justice framework would dictate compensation for the Lacks family and a strategy to reform medical research so that research subjects, particularly those whose bodies were historically used for others’ profit, would be assured of enjoying the benefits of the research.
Following the publication of Rebecca Skloot’s 2010 book on Henrietta Lacks, her descendants established a foundation to “preserve her legacy by educating future generations on the impact of her phenomenal HeLa cells while promoting health equity and social justice.” In fact, August 1, 2020 marked the beginning of a year’s “Cellebration” of the 100th anniversary of Henriette Lacks’s birth. Today, February 14, 2021, the day of this blog post, the foundation suggests a donation of $14 as a “V-Day gift.” It is also worth noting that the foundation actually advocates for receiving the COVID-19 vaccine as a way to honor the legacy of Henrietta Lacks.
Similarly, those who wish to decrease the number of abortions might also consider a Restorative Justice approach. All birthing people, but especially people of Color, who are disproportionately represented among people terminating pregnancies, should be guaranteed sufficient health care access and financial support so that those who wish to do so can carry their prenates to term and parent all their children in safety and with dignity. Data from the Guttmacher Institute, as reported by CBS News, suggest that the inability to afford a baby is a reason for 73% of women who obtain abortions. Obviously, the fate of prenates who were not carried to term cannot be changed. But the fate of birthing people can. It would make sense for everyone, whatever their position on abortion, to support organizations that fight to improve circumstances for birthing people and their children, like Mothering Justice, Black Mamas Matter Alliance, and others.
One moral concern?
Finally, regardless of the utility of boycotts and the application of a restorative justice lens to problems of fairness and equality, is there ever a world in which one moral concern can override all others? You might believe, for example, that your cause in life is to save elephant species from extinction. They are beautiful, intelligent animals, and you are sure they have souls. You might feel moved to decline a vaccine because it was created using, say, cells from elephant ivory,3 which poachers obtain by killing the animals. But to ignore all other issues – climate change, political unrest, or a world pandemic, perhaps? – not only means that an opportunity to save the elephants might elude you, but also suggests a lack of connectedness to the larger world. Friends, the world needs many things. We our connected to our natural world and to one another. Please, let us consider multiple viewpoints and multiple approaches for our mutual aid.
Updated June 9, 2021: graphic replaced and small stylistic changes made
1The Common Rule (45 CFR part 46), the Federal Policy for the Protection of Human Subjects, was established in 1991. It is enforced by research institutions through Institutional Research Boards. Note that the Common Rule applies only to medical research, not medical practice.
2“Restorative justice began as an effort to deal with burglary and other property crimes that are usually viewed (often incorrectly) as relatively minor offenses. Today, however, restorative approaches are available in some communities for the most severe forms of criminal violence: death from drunken driving, assault, rape, even murder. Building upon the experience of the Truth and Reconciliation Commission in South Africa, efforts are also being made to apply a restorative justice framework to situations of mass violence. These approaches and practices are also spreading beyond the criminal justice system to schools, to the workplace and religious institutions. Some advocate the use of restorative approaches such as circles as a way to work through, resolve and transform conflicts in general.” Zehr, Howard. The Little Book of Restorative Justice: Revised and Updated. New York: Skyhorse Publishing Company, Incorporated, 2015. See also “Restorative Justice as a Social Movement,” in Mark Umbreit and Marilyn Peterson Armour, Restorative Justice Dialogue: An Essential Guide for Research and Practice, 2010.
Frames 2 and 3: The following images were cropped and speech bubbles were added. We do not imagine that the thoughts we have attributed to the people shown represent what they were actually thinking. The attribution for all images in Frames 2 and 3 is “45th MARCH FOR LIFE RALLY on the National Mall between 12th and 14th Street and Jefferson and Madison Drive in Washington DC on Friday morning, 19 January 2018 by Elvert Barnes Protest Photography.”
Click the image to open a larger version in a new window.
An Epidemic of Home Birth?
As if the U.S. maternity care system didn’t have enough challenges to deal with – a spot of obstetric violence here, a 4-fold racial disparity in maternal mortality there – now there’s that dang Coronavirus! It should come as no surprise that both hospitals and pregnant people might now find themselves with qualms about the practice of giving birth in hospitals.
One potential objection is that healthy people about to give birth might be wary of doing so in a place filled with sick people with a highly contagious disease. The other concern, from the hospital’s point of view, is that facilities and providers might well be strained to the maximum by the exigencies of caring for pandemic patients.
As a result, even parents-to-be who would not have chosen home birth before might find themselves considering it now. It’s not a bad idea! A majority of pregnant people are healthy and are good candidates for home birth. (For comparable safety data on place of birth, see our post here for starters. For more recent data, see the just-released Birth Settings in America report or this summary.) We won’t pretend that hospital-based experts recommend home birth, but others have weighed in on the benefits of separating out healthy mothers and babies from COVID-19 sufferers. None of this is news: in past epidemics, some pregnant hospital patients have switched their planned place of birth.
In order to make out-of-hospital birth possible for many families, however, appropriate providers must be found to attend those births. The good news is that midwives, particularly Certified Professional Midwives, are currently practicing in almost every state. How those states facilitate access to that care is another matter. CPM practice is legally authorized in 35 states, but each state has different views on CPM scope of practice, Medicaid coverage, and many other issues. In the remaining states, CPM practice exists on a spectrum from unregulated to illegal status.
If ever there were grounds for support of these maternity care providers who specialize in out-of-hospital care, the COVID-19 pandemic provides it. States must use the emergency police powers available to them to facilitate access to CPMs, and hospital-based medical providers must turn to the important work that only they can do and stop opposing what pregnant people want: the option to give birth in the place of their choosing, attended by a provider of their choice.
Image credits
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.
Frame 2: The car racing to the hospital is from a photo on ph.
Frame 3:The ultrasound scene is by artistraman. The busy hospital exterior is a cropped version of a photo by PAspecialNHCL.
Frame 4: The messy dining room is by Hans. The pregnant woman is by readingruffolos. The child with fingers in his nose is by ranjatm.
Frame 5:The bedroom is from pxfuel. The doctor is by OpenClipart; the image is in the public domain. The hand reaching for the button is selected from an image from pxfuel. Helper midwife is cropped from a photo from AllGo. The red carrying cases at her feet are by Dids. The wall portrait is by pxfuel, as is the children’s drawing. At the head of the bed, the map of licensed states is from The Big Push for Midwives; a larger copy is included in the blog text above. The primary midwife is by Tosha Noakes.
Click the image to open a larger version in a new window.
The last few years have seen an increase in states working to decriminalize recreational marijuana use by adults. Apparently, the U.S. Surgeon General believes that only illegal status was preventing pregnant people from puffing their nine months away, because this year he issued a strong warning against marijuana use during pregnancy.
This cartoon addresses criminalization of marijuana use rather than a generalized warning, but the fact is that laws that criminalize drug use during pregnancy and issue special penalties for it already exist and women are being charged under them. Furthermore, even in decriminalized states, mothers still face consequences for marijuana by way of the child welfare system; sanctions can include one that many mothers would rate even worse than the loss of their liberty: the loss of their child. These repercussions seem vastly disproportionate to the drug-using behavior, considering the following facts:
The effects of marijuana use during pregnancy are often overstated in the absence of concrete data.
The effects of marijuana use during pregnancy are often confounded with other substance use – including alcohol and tobacco, which are far more dangerous to the baby than any illicit drug.
The effects of marijuana use during pregnancy are often confounded with socio-economic status and with disparate effects by race, including uneven enforcement, uneven consequences, and uneven expectation of privacy. Indeed, the effects of intervention itself in the form of child welfare agencies cannot be classified as benign; certainly, separating babies from their mothers in the first hours of life isn’t good for either party.
Sanctions, whether threatened or real, scare pregnant people away from prenatal care. When so many things in our lives are bad for babies (job loss, environmental pollution, violence against women), this fixation with a substance whose harm hasn’t even been fully established looks like just another way to criminalize pregnancy. In addition, when marijuana use is legal, punishing users might serve as the bridge to criminalizing tobacco and alcohol use. Or consumption of runny cheese! Or hot tub use. … Or living in a neighborhood where the water has been turned off, homes have been foreclosed upon, and the factory next door belches a queasy-making smoke that the municipality assures residents is Perfectly Safe.
If we want pregnancy to result in healthy babies and healthy mothers, perhaps we might concentrate on known dangers and support parents in ways that don’t involve a) a jail cell, or b) the threat of separation on the single most important day in a brand-new person’s life.
Suggested reading
Khiara M. Bridges, The Poverty of Privacy Rights (Stanford, California: Stanford Law Books, 2017).
Frame 5: The photo is by Patricia Deal, and is in the public domain. Because this photo portrays a real person, we wish to emphasize that the pregnant woman pictured did not speak the words we put in her mouth. In no way do we wish to suggest that the circumstances suggested by those words apply to her.
This post was conceived with the help of The Big Push for Midwives, which also helped out with its delivery.
Click the images to open a larger version in a new window.
Private Membership Associations
Earlier this year, news articles reported on criminal actions against community (out-of-hospital) midwives in Indiana and Nebraska following infant deaths. More recently, the work of one midwife in Minnesota was highlighted; she was not under state investigation, nor were any bad birth outcomes mentioned.
What do these three midwives have in common? They all have formed Private Membership Associations (PMAs), legal instruments that claim to exempt their members from state regulation. Clients of these midwives become members of PMAs, which supposedly allow them to essentially contract out of state governance of their midwives.
However, in reality it doesn’t work that way. States with licensing regimes, like Indiana, allow their state midwifery boards to issue complaints against negligent midwives, whether the midwives have obtained licenses or not. Because the unlicensed practice of a profession is a criminal offense, these complaints are often conveyed to the state attorney general’s office, after which charges may be filed against the midwife. In states that do not offer licensing of community midwives, like Nebraska, the route to criminal charges is much more direct: reports of a bad outcome may land immediately on the county prosecutor’s desk.
The cartoon above is our take on why PMAs are a bad idea, and why midwife licensing is a good idea. Many people these days mistrust government – and who can blame them? But remember: the answer to bad law isn’t no law; the answer to bad law is good law.
An aside about PMAs, birth outcomes, and midwife arrests
When midwives are arrested after a newborn or maternal demise, as in the news articles linked above, some readers find it tempting to channel their lock-em-up-and-throw-away-the-key rage right at them. Allow us to take this opportunity to remark that physicians rarely face arrest when their patients die. Furthermore, this post is in no way a comment about the outcomes in any of the births in the news articles or on the level of skill and training possessed by the midwives who attended those births. Midwives are often blamed for bad birth outcomes no matter what their license status, training, skill, or education. The shamefully high infant and maternal mortality rates associated with conventional hospital-based care, on the other hand, is just starting to be questioned.
Image credits
All images are shared under a Creative Commons license, unless otherwise noted. Where required by license, changes to the image are noted.
The sailing ship is a photograph of Cannon Fired by Willem van de Velde the Younger, 1707. The photo is by the Rijksmuseum, Amsterdam and is in the public domain.
The Virginia-class attack submarine is by Owly K. The photo is in the public domain.
The cannon is from a photo of the Saint Kitts – Brimstone Hill Fortress, taken by Martin Falbisoner.
Panel 3
The background is a photo of the Ballroom at Rideau Hall, Ottawa, by Dennis Jarvis. We cropped the image, edited out some chairs along the back wall, and swapped the portrait of Her Majesty Queen Elizabeth II with one of Martha Ballard, midwife.
The lectern is from “WikiData Presentation 2018,” by Michelle Nitto.
The pink house in the poster is of Zemīte Manor, by J. Sedols.
The midwife/breastfeeding mother is by Renoir. She is wearing an oxytocin necklace. Her bag is from Needpix.com. It is filled with a water bottle by wraithrune, a yoga mat by MikesPhotos, and a sweet little stuffed cow by OpenClipart-Vectors.
Finally, the speaker at the lectern is Cynthia Jackson, CPM, LM, of Michigan: midwife extraordinaire and unparalleled portrait subject. The photo is used with permission. Ms. Jackson runs Sacred Rose Birthing Service and is a founder of the Mosaic Midwifery Collective, both in Detroit.
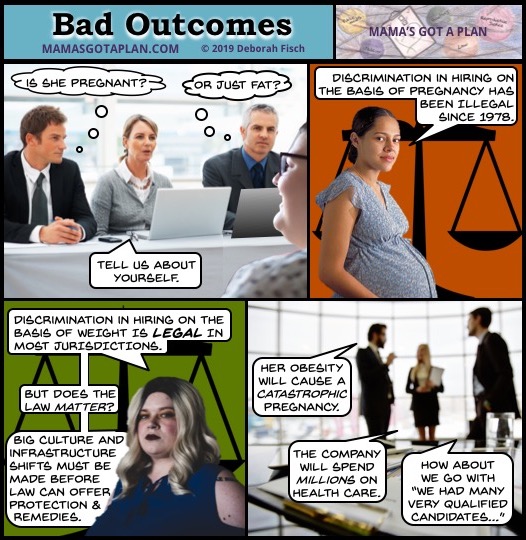
Some women1 are pregnant. Some women are fat.2 Some women are fat and pregnant. Almost all of these women need jobs, the same as anyone else. Employment discrimination in hiring is sadly not unknown to many would-be employees, but the fat-and/or-pregnant job-seeker encounters specific additional challenges.
Pregnant?
The Pregnancy Discrimination Act of 1978 forbids employment discrimination on the basis of pregnancy, considering it a form of sex discrimination. The strongest protections apply to the hiring process, but are difficult to access unless an employer documents their decision to discriminate. Employers are not allowed to ask applicants if they have children, plan to have children, or are currently pregnant. Of course, at a certain point a pregnancy becomes visible – unless it is mistaken for fatness.
Fat?
Discrimination faced by fat people is widespread. Fat people are seen not only as failures at controlling their body size, but also as generally untrustworthy, incompetent, and unhealthy. Most U.S. jurisdictions offer no legal protection against weight-based discrimination in employment or any other context. Even if legal protection were available, remedies might remain elusive should traditional code words for overlooking fat applicants be used: “unprofessional appearance” or “incompatible with company image.” Now for the double whammy …
Fat AND pregnant?
Yes, Virginia, fat people get pregnant and have babies! It is in these circumstances that employers fall prey to the particularly injurious prejudices about fat people, who are so often characterized as being “one cheeseburger away from a fatal heart attack.” Imagine if a fat person is also pregnant! It’s practically a death sentence! This rate of fatality would be highly inconvenient to employers – not to mention the fat person herself – if it were true.
There are higher risks of some complications of pregnancy associated with higher body weights, but that is true of other (visible) conditions as well: very low body weight, twin or multiple pregnancy, and pregnancy for African-American women, whose maternal mortality is tragically 3-4 times that of white women. The scientific evidence is finally beginning to concede that higher mortality for the African-American population is not the result of race, but of racism. The role of bias and stigma may also be behind the associations of certain types of risk with bad outcomes for fat pregnant women. Regardless of the science, the popular perception is as stated in Frame 4: hiring a pregnant fat woman will bankrupt your business through high health care costs3 when her pregnancy inevitably goes south.
Why do these beliefs persist?
The cultural understanding of women’s participation in the workplace remains far from settled, at least when women take valued positions previously held exclusively by men. Even women who are not pregnant or incapable of becoming pregnant can suffer from employer suspicion that members of the sex that “naturally” acts as family caretakers are likely to be called to do just that, to the detriment of their jobs. Applicants who are pregnant are felt to be freeloading: if other new employees are not permitted to take leave until they have put in the required amount of time, why can babymakers? They should have kept their legs closed!
As for fat pregnant women, well, should they really be permitted to reproduce? Not only will they almost certainly harm their babies and themselves in the process, draining company and public health dollars at an alarming rate, but they might produce more little fat people. A job would just encourage them!
While these last paragraphs are increasingly sardonic in style, they serve to illustrate the result of combining over a century of anti-fat bias, medical eagerness to believe that fat is the cause of all ills, pressure on businesses to reduce health care spending, an economic framework that blames the need of the human race to reproduce on the people doing the reproducing, and a general lack of understanding that we are all in this together. And this moral mess hasn’t even begun to address the additional and intersectional issues encountered by people of color, LGBTQ people, people with disabilities, or immigrants.
“I want to do the right thing – what is it?”
You don’t really need us to tell you, do you? Stop discriminating!
Admittedly, it’s not that simple. However, like charity, abuse begins at home – and that’s a good place to stop abusing your fat friends and family members. Even if you’re doing it because you’re “concerned for their health.” Especially then.
Then take up the standard in your workplace. Make sure that both pregnant and fat people are accepted as full members of the workforce. If you are responsible for hiring, then you are especially positioned to make change. Finally, when the common beliefs about fat and/or pregnant people begin to budge, work with policymakers to forbid this kind of discrimination.
1We usually use the phrase “pregnant people” or “birthing people.” However, because the topic of this cartoon is extremely gendered, we will refer to “women,” with the understanding that pregnant people who do not identify as women face additional problems beyond the scope of this post. 2The accepted medical term these days seems to be people who “have obesity.” We use “fat” as the term preferred by the fat acceptance movement. 3Obviously, the structure of the U.S. health care payor system is a key culprit in employers’ general fears about health care costs. This post is not trying to solve that problem. One thing at a time, okay?
Bibliography
Pregnancy discrimination in the workplace. Maren Thomas Bannon, “How Can We Talk about Workplace Equality When We Still Punish Women for Getting Pregnant?,” Quartz, accessed September 17, 2019, https://qz.com/1686054/we-cant-talk-about-workplace-equality-when-we-still-punish-women-for-getting-pregnant/. This article gives an overview of employment penalties faced by female venture capitalists – an elite group. Imagine the hardships faced by hourly workers who need permission for bathroom breaks!
Stigma and health disparities. Mark L. Hatzenbuehler, Jo C. Phelan, and Bruce G. Link, “Stigma as a Fundamental Cause of Population Health Inequalities,” American Journal of Public Health 103, no. 5 (May 2013): 813–21, https://doi.org/10.2105/AJPH.2012.301069.
African-American Birth Outcomes.Fleda Mask Jackson et al., “Examining the Burdens of Gendered Racism: Implications for Pregnancy Outcomes Among College-Educated African American Women,” Maternal and Child Health Journal 5, no. 2 (June 2001): 85–107.
We are very pleased to announce that our 20-page booklet, Pushed and Consented: Rights in Childbirth?, is available for purchase on the Birth Rights Bar Association website. Click the cover image to go straight there!
Cartoons with explanatory text address the question mark in the title and lay out the current legal landscape. Buy your copy today!
If you would rather view the booklet online, it is available at this link. BRBA suggests making a donation if you choose view the booklet online.










 Some people with concerns about the safety or efficacy of vaccines object to the presence of “aborted fetal cells” in vaccines. However easy (and gruesome!) it is to picture a dismembered hand pushing up through a syringe’s liquid, that is not the reality. As the blue-jacketed person in Frame 3 tries to point out, what is in question are cell lines. How are cell lines formed? Scientists use cells taken from
Some people with concerns about the safety or efficacy of vaccines object to the presence of “aborted fetal cells” in vaccines. However easy (and gruesome!) it is to picture a dismembered hand pushing up through a syringe’s liquid, that is not the reality. As the blue-jacketed person in Frame 3 tries to point out, what is in question are cell lines. How are cell lines formed? Scientists use cells taken from  an organism, e.g. kidney cells taken from a dead human embryo, and create a replicating cell line. The original kidney cells eventually die off, just as cells in the body do, and are replaced by genetically identical cells created by standard biological cell division. These cells are then combined with viruses and used to create a vaccine. (For fascinating photos of human embryonic stem cells, see
an organism, e.g. kidney cells taken from a dead human embryo, and create a replicating cell line. The original kidney cells eventually die off, just as cells in the body do, and are replaced by genetically identical cells created by standard biological cell division. These cells are then combined with viruses and used to create a vaccine. (For fascinating photos of human embryonic stem cells, see 
 Other wrongs, however, remain to be righted: consider the case of Henrietta Lacks. The HeLa cell line was developed from cells taken from the cervical tumor that killed Lacks in 1951. The line has been successfully used for far-reaching discoveries in cancer drugs, space research, and immunology, including in the study of COVID-19 in search for a vaccine. The moral issue arises from the fact that while great good came of the establishment of the line, none of that good was directed specifically toward the Lacks family.
Other wrongs, however, remain to be righted: consider the case of Henrietta Lacks. The HeLa cell line was developed from cells taken from the cervical tumor that killed Lacks in 1951. The line has been successfully used for far-reaching discoveries in cancer drugs, space research, and immunology, including in the study of COVID-19 in search for a vaccine. The moral issue arises from the fact that while great good came of the establishment of the line, none of that good was directed specifically toward the Lacks family.

 Finally, regardless of the utility of boycotts and the application of a restorative justice lens to problems of fairness and equality, is there ever a world in which one moral concern can override all others? You might believe, for example, that your cause in life is to
Finally, regardless of the utility of boycotts and the application of a restorative justice lens to problems of fairness and equality, is there ever a world in which one moral concern can override all others? You might believe, for example, that your cause in life is to 
 be found to attend those births. The good news is that midwives, particularly Certified Professional Midwives, are currently practicing in almost every state. How those states facilitate access to that care is another matter. CPM practice is legally authorized in 35 states, but each state has different views on CPM scope of practice, Medicaid coverage, and many other issues. In the remaining states, CPM practice exists on a spectrum from unregulated to illegal status.
be found to attend those births. The good news is that midwives, particularly Certified Professional Midwives, are currently practicing in almost every state. How those states facilitate access to that care is another matter. CPM practice is legally authorized in 35 states, but each state has different views on CPM scope of practice, Medicaid coverage, and many other issues. In the remaining states, CPM practice exists on a spectrum from unregulated to illegal status. 







{kind=link}
.jpg){kind=link}
#/media/File:Rally1.MFL.NationalMall.WDC.19January2018_(25917155088).jpg){kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}